What Killed Michael Clark?
The official Travis Co. autopsy doesn't tell the whole story
By Jordan Smith, Fri., Dec. 2, 2005





Photo courtesy of Jeff Clark
Just after 1pm on Sept. 26, the second of two record-breaking 108-degree days, Austin police officers working the department's Southeast Area Command responded to a call for service on East William Cannon Drive. When they arrived, they found 33-year-old Michael Clark involved in an altercation with an as-yet-unidentified woman. According to an APD press release, Clark was "displaying behavior that was violent and irrational." As the officers tried to arrest him for public intoxication, he threatened them and fought with them, biting Detective Robin Denton on the hand and injuring Sgt. Robert Pewitt's shoulder. Eventually nine officers were on the scene and at least two used weapons on Clark, spraying his face with pepper spray and striking him three times with a Taser – twice in the chest and once in the arm – before they were able to subdue him. Once Clark was under control, the officers sat him upright – department procedure whenever a Taser is used – called EMS, and poured water on him, to cool him down in case he was overheated, reported Travis Co. Deputy Medical Examiner Elizabeth Peacock, and Clark seemed to be breathing fine. But that didn't last; according to APD, shortly after he was taken into custody, Clark went into "medical distress" and was transported by EMS to South Austin Hospital. At 3:55pm he was pronounced dead.
Most details of the incident – recorded by APD in-car video cameras, and in police, EMS, and hospital reports – remain under seal by the APD, because officers are still reviewing the incident, standard procedure for any police-related death. The two officers who fired their Tasers at Clark – officers Douglas Drake and Blaine Eiben – were placed on restricted duty immediately following the incident, but after an initial review by police investigators, they were returned to the street just two days later. "It appears to us the officers followed the [use-of-force] policy that we have established," Assistant Chief Cathy Ellison told the Statesman on Sept. 29.
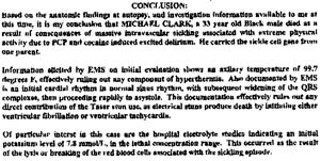
Nonetheless, Michael Clark was dead. It was more than a month before the ME's office released Peacock's autopsy report, signed on Oct. 28 but performed the day after his death. According to Peacock, Clark died as a "result of consequences of massive intravascular sickling associated with extreme physical activity due to PCP and cocaine induced excited delirium." (As a consequence of "sickling," or collapsing, red blood cells lose oxygen, and the liquid hemoglobin they contain becomes a gel-like substance, due to a genetic disorder known either as sickle cell anemia or sickle cell trait, the two forms of the disease.) In other words, according to Peacock, Clark was high and became agitated and "delirious" enough to cause his blood to lose oxygen, which in turn caused the red blood cells to sickle, killing him.
Moreover, Peacock appeared determined to exclude absolutely any external contributing causes to the fatality. She concluded that neither the Taser strikes nor the heat of the day contributed, in any way, to Clark's death. Clark's body temperature – taken under his armpit at the scene by EMS – was just 99.7, "effectively ruling out any component of hyperthermia," Peacock wrote. And an initial cardiac test, also taken by EMS, showed "normal sinus rhythm," ruling out any "direct contribution of the Taser," which according to the ME would have produced a spiking, rapid heartbeat.
Clark's family and supporters, including Nelson Linder, president of the Austin chapter of the NAACP, have not accepted Peacock's findings, and they do not believe that Clark's death was caused either by blood-cell sickling or by drugs. Instead, they suspect that it was caused by the police use of force, and most specifically, by the repeated Taser strikes. "There are lots of inconsistencies [in the autopsy report]," says Linder, and "we feel very certain" that sickling did not cause Clark's death.
Nonetheless, Peacock is adamant: Red blood cell sickling killed Clark – not the Taser or the heat. In the course of preparing her autopsy, Peacock says she reviewed videotapes of the event, read EMS and hospital reports, and even had police go back out to the scene the next day to take temperature readings, to determine how hot the concrete and a patrol car had been. "Had it not been for the sickling, [Clark] would be alive today," Peacock said in a phone interview. "I've gone to medical school, I saw the tapes, and that's my conclusion."
Click for a larger image
But Clark's family members aren't the only ones skeptical of that conclusion. Indeed, medical experts asked by the Chronicle to review the Clark autopsy – including doctors, genetic researchers, and forensic pathologists – all say they don't believe sickling caused Clark's death, and several doubt that he died from drug-induced delirium. What they don't know, they said, is what did kill Michael Clark. "There are lots of unanswered questions," says Dr. Oswaldo Castro, acting assistant director of the Center for Sickle Cell Disease research at Howard University in Washington, D.C.
The Suspect Sickle Cells
For the record, sickle cell trait and sickle cell anemia are not the same thing. Each is a form of sickle cell disease, a genetic disorder, but they are not equally severe. People with sickle cell trait carry a single defective gene – from either mother or father – and while they are carriers of the disease, people with sickle trait typically live a symptom-free life, says Dr. William Winter, acting director of the Center for Sickle Cell Disease research at Howard University. In contrast, people with sickle cell anemia carry two defective genes, and typically manifest a host of problems, from joint pain to kidney disease. In her autopsy report, Peacock noted that Clark carried a "sickle cell gene from one parent," meaning he was living with sickle cell trait. (Unfortunately, both the APD and the local press incorrectly interpreted Peacock's findings, reporting that Clark had sickle cell anemia.)
The difference between the two forms of the disease is important, experts say, because it is extremely rare that a person carrying the sickle cell trait would ever "keel over and drop dead from sickling" – even under "extreme" conditions, says Winter, such as flying in an airplane that is not adequately pressurized. Perhaps more important, however, is the fact that death itself always causes sickling in red blood cells, even in a person with no genetic disorder. As such, experts say, finding sickling after death is in no way indicative of how or why a person died. "It's extremely unusual for people to die of sickle cell crisis under any circumstance," says Dr. Michael Baden, the star of the HBO series Autopsy (and in the 1970s, chair of the congressional panel reinvestigating the deaths of President John F. Kennedy and civil rights leader Martin Luther King, Jr.). Moreover, Baden continued, "Finding sickle cells at autopsy doesn't mean anything."
Delirium or Hypoxia?
Also problematic, says Baden, is Peacock's determination that the allegedly fatal sickling event was brought on by drug-induced "excited delirium," an increasingly cited but somewhat controversial cause of death, most often applied to cocaine users who die suddenly while in police custody. The American Medical Association does not recognize excited delirium as a diagnosable disease or syndrome, but the condition, while not well defined, has been around for more than 20 years, and is accepted by the National Association of Medical Examiners. "It is a very rare situation that happens when you take cocaine," said Baden. Within 30 minutes of using cocaine – the window of time for the drug's peak effects – the user becomes agitated, combative, and wild, as "your temperature shoots up to 109 degrees and you die," Baden said. (Exactly why some, typically chronic, drug abusers die from excited delirium is unknown, but some researchers theorize that it is caused by increased adrenaline and dopamine production that becomes a lethal cocktail of naturally occurring body chemicals.)
But Clark didn't have cocaine in his bloodstream, only its metabolite in his urine, meaning he wasn't under the influence of cocaine at the time of his death. (Cocaine is generally flushed from the bloodstream within 24 hours.) And Baden says he isn't aware of any cases of PCP-induced excited delirium. Moreover, the fact that Clark's temperature was just 99.7 degrees immediately following his confrontation with police also tends to rule out excited delirium as the cause of death, he said. "If he'd had excited delirium, [his] armpit temperature should [have been] around 106-107."
Although Baden is hesitant to draw any hard conclusions without reviewing the police videos and the EMS and hospital reports, he suspects that Clark's death may in fact have been caused by something far less exotic than either sickle cells or excited delirium. Instead, Baden says it's far more likely that Clark died from hypoxia – a loss of oxygen – brought on by the pepper spray, Tasers and, perhaps, police handcuffing technique. "The most common way someone dies in this [type of] situation is from [someone] sitting on the [person's] back while handcuffing them," he said. "This is a concern because pepper spray ... prevents [a person] from breathing properly, as do Tasers. [So, from the drugs] he gets disoriented and argumentative, and what he is, is a mental health problem," he continued. "If [Clark] had not had this encounter with the police, he wouldn't have died – not from the high temperature, not from the sickle cell, [not from] the argument."
Adding the Taser
Do Tasers kill? If so, how? Those two questions are at the heart of the ongoing debate over police use of the electroshock Taser gun. More than 8,000 law enforcement agencies in 43 countries have added Tasers to their arsenals, and many departments credit the weapon with decreasing injuries and reducing the number of potentially lethal police confrontations. In April, APD Chief Stan Knee reported to council that APD use of Tasers has led to a marked reduction in injury to both officers and suspects – a decrease of 53% and 80%, respectively – and a reduction in the number of complaints of excessive use of force by police – down from 36 in 2002 to 27 in 2004.

Still, not everyone is delighted with the proliferation of the Taser, and several human-rights organizations, including Amnesty International, have called for a moratorium on their use, arguing that research into the effects of the Taser's 50,000-volt shock are, at best, inconclusive and that police policies governing their use are inconsistent and insufficient to protect against abuse. Electroshock weapons, like those manufactured by industry leader Taser International, are not regulated by any governmental agency, and there are no universal manufacturing standards. Moreover, there has not been any government-sponsored research on the health effects of electroshock weapons since 1976, when the U.S. Consumer Product Safety Commission concluded that the weapon's electric charge "would not be expected to kill a normally healthy adult," but that "persons especially sensitive to electric shock could be at risk."
While the CPSC's conclusion – echoed in recent years by subsequent research – may be unsatisfying, it's hard to determine the specific physiological effects of a Taser strike, says Tarrant Co. Deputy Medical Examiner Lloyd White. The 50,000 volts delivered during a five-second Taser strike alone is not enough to kill, White said, but the weapon does appear able to set off a fatal chain of events in some people – especially those with drugs in their system. "There have been 100 and some Taser deaths documented ... and virtually all of them have coke or meth on board," he said. "We've had four or five this year, [and it's interesting to see] how many are related to multiple Taser shots. That's the biggest source of controversy." Moreover, the standard five-second strike by a Taser fired from a distance may not be the only procedure worth reviewing; a handheld Taser applied directly by an officer is capable of delivering an ongoing shock much longer in duration than five seconds.
Indeed, in June, Taser International issued a training bulletin, warning that "[r]epeated, prolonged, and/or continuous exposure(s) to the [Taser] electrical discharge may cause strong muscle contractions" that could "impair breathing ... particularly when the probes are placed across the chest or diaphragm." Further, according to the bulletin, when dealing with individuals exhibiting signs of excited delirium, police should be careful to use the Taser in combination "with physical restraint techniques to minimize the total duration of the struggle and minimize the total duration of [Taser] system stimulation." The company issued the bulletin, in part, because it "has come to our attention that there may be a training issue where [police] are avoiding touching the subject [of the use of force] during the Taser application," the bulletin reads – meaning, apparently, that instead of taking advantage of the Taser-induced incapacitation, some officers were waiting to move in to cuff the suspect until after the jolt was complete, thereby necessitating repeated strikes.
Taser foes quickly pointed to the report as evidence that the Taser is more dangerous than the company had previously led the public to believe. Not true, says Steve Tuttle, Taser International's vice-president of communications. The point of the bulletin was to provide additional information that could be helpful in building law enforcement Taser-use policies, Tuttle said, and not to suggest that the Taser is lethal. "If we found evidence in medical testing that would lead us toward [that conclusion, we would say so]," Tuttle says. "In fact, [Tasers] are not risk-free at all. We've been in the forefront of that too. The first manual we put out said, 'Watch out: These can put an eye out!'"
And although Taser foes claim that more than 100 people have died after being shocked with the weapon, Tuttle notes that the Taser has been cleared as the cause of death in almost every case. In fact, he said last month, by the second week in November the Taser had already been "cleared" in three recent deaths – including Clark's.
Open Questions
Clark's family isn't as convinced as Tuttle and Peacock that the Taser played no part in Michael Clark's death, says Nelson Linder, who has secured an outside expert to review Peacock's work in the case. Questions in the Clark case are not likely to be resolved by Peacock's categorical refusal to consider contributing factors to Clark's death. And it doesn't help that the Travis Co. Medical Examiner's Office has made several recent, high profile errors – including a botched toxicology testing in the emotionally charged police shooting death of Daniel Rocha. In October, county commissioners ordered an audit of the office that will focus on medical practices and procedures. (For a list of recent cases in question, see "Trouble at the ME's Office," below.)
On the day the Clark autopsy was released, APD officials issued a brief press statement, noting that the department "continues to believe that the proper use of Tasers is critical to ensure situations are resolved with minimal injuries to officers and suspects," and pointing out that Peacock ruled that Clark's death was "accidental" and "did not result from the deployment of Tasers by officers." Nonetheless, in the same statement, the department announced that City Manager Toby Futrell has asked EMS Medical Director Ed Racht to "develop a committee of local medical professionals to research the medical implications associated with the use of Tasers." In the intervening weeks, Futrell's directive resulted in an upcoming conference of medical directors, physicians, and academics from across the nation – including Racht's counterparts in Chicago, San Francisco, Nashville, New York, Houston, and Dallas – who will converge in Austin on Dec. 8-9 to "review the clinical literature, the medical literature, [and] the published data," Racht said recently, related to the medical effects of Tasers. The goal, Racht said, will be to help "our communities" understand the medical implications of Taser use.
"All of us, clinically, are struggling with the same issues," says Racht. "It's an emotionally charged issue, a clinically charged issue, that is important to all sides." Racht said the panel of medical professionals hope to come up with a set of medical recommendations "that [we] can take back to [our] communities and start doing the best we can." Moreover, Racht said that this week, independently of the police department, a panel of five local medical experts – including Racht as well as Peacock – plans to convene to review the record on Clark's case in particular, in an effort to try to understand the "medical implications" of Clark's death. Racht said the panel's findings will be made public. "The purpose," he said, "is to let the public know" why Clark died.
And that, says Dr. Baden, is an admirable goal that should also help police better do their job – "The police are equally being misled by a diagnosis of sickle cell," he said. "They assume that is correct." ![]()
Got something to say on the subject? Send a letter to the editor.



